


Prescribing IV fluids: types of fluid
IV fluid summary for medical student finals and OSCEs
- Fluids are one of most frequent in-hospital prescriptions.
- For exams you will need to know the approximate fluid volumes in each compartment and the requirements in a 24-hour period
- Examination of fluid status is also important in assessing what fluid type and rate to prescribe (click here to learn how to do it)
Fluid compartments
- Intravascular: 5L (1/9 total)
- Interstitial: 9L (2/9 total)
- Intracellular: 28L (2/3 total)
NB. Fluids are given intravenously and, hence, are added to the intravascular space. However, a certain proportion of the water content will be distributed across all of the fluid compartments (intravascular, interstitial, intracellular). The rate that IV fluids distribute depends on the osmotic gradient that they create intravascularly. Colloids>saline>Hartmanns>dex-saline>dextrose (with colloids staying intravascularly the longest and dextrose the shortest).
Normal fluid requirements (i.e. maintenance fluid requirements if no oral intake)
- Fluid requirements depend on the patient’s weight.
- For a 70kg patient over 24 hours:
- Water: 2.5L (1.5ml/kg/h)
- Sodium: 70-140mmol (1-2mmol/kg/24h)
- Potassium: 35-70mmol (0.5-1mmol/kg/24h)
Urine output
- Urine output (UOP) should be >0.5ml/kg/h
- For a 70kg patient this is: 35ml/h
Composition of different IV fluids
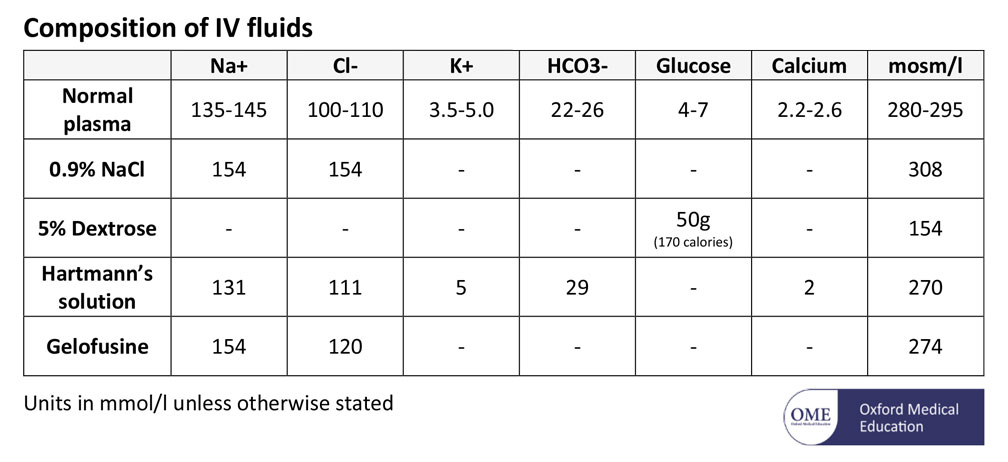
Components of IV fluids – saline, hartmanns, dextrose, gelofusine
Types of IV fluids
5% dextrose
- 5% dextrose is given instead of pure water (the glucose is used up) to maintain initial osmolarity. The glucose content plays no role whatsoever (the calorific content is negligible)
- Good
- It is used for maintenance to give water when needed with no electrolytes
- Useful as maintenance fluid (alternating with 0.9% saline in those with normal electrolytes)
- Can add 20-40 mmol KCl a 1L bag as needed
- Bad
- It has no place for replacing plasma/blood loss because it is not physiological.
- Too much too quickly causes hyponatraemia
Normal 0.9% saline
- Normal saline (0.9% saline) contains the salts sodium and chloride. This makes it more physiological (closer to plasma) than dextrose but not as physiological as Hartmann’s solution.
- Good
- Useful as maintenance fluid (alternating with 5% dextrose in those with normal electrolytes)
- Can add 20-40 mmol KCl a 1L bag as needed
- Bad
- Too much too quickly causes hypernatraemia
- Only using saline as maintenance can be renotoxic: it puts a massive sodium load on the kidneys and can cause renal vasoconstriction
- Can give a hyperchloraemic acidosis (HCI <=> H+ and CI-)
Hartmann’s solution
- Hartmann’s solution is the most physiological (i.e. similar to plasma) fluid available
- Good
- Excellent for replacing plasma loss e.g. during surgery or GI losses
- The anaesthetists’ choice!
- Bad
- Shouldn’t be used as maintenance alone: 3L Hartmann’s solution over 24 hours would give 3 times too much sodium and not enough potassium.
- Cannot add extra potassium or magnesium to the bag
Dextrose -saline
- Dextrose-saline contains some dextrose and some sodium chloride
- Good
- Good maintenance fluids as it contains approximately the correct requirements of sodium
- Bad
- It has no place for replacing plasma/blood loss because it is not physiological
- Too much too quickly can cause hyponatraemia
Colloids
- Colloids contain large molecules which stay intravasculary and create an osmotic gradient. Types include starches (valvuven/volylyte), gelatins (gelofusine), albumins
- Good
- Acutely in small volumes when you need to keep fluid in intravascular space (e.g. fluid challenges)
- However, there is very little evidence they are better at this than crystalloids
- Acutely in small volumes when you need to keep fluid in intravascular space (e.g. fluid challenges)
- Bad
- Not as inert as crystalloids and can (very rarely) cause anaphalaxis and renal failure
- NICE do not routinely recommend their use in any situation
Additives
- Electrolytes can be added to bags of saline or dextrose as required
- Click here fore notes on how to replace electrolytes
- NB. There are pre-made versions of saline, dextrose and dextrose saline with different concentrations of potassium (20mmol or 40mmol)
Now click here to learn how to prescribe the fluids above, and click here for how to examine for fluid status
Perfect revision for medical student finals, OSCES and PACES
For further reading, click here for notes on shock in emergency medicine